Multifactorial Disorders: Cleft Palate/Lip
What are multifactorial/complex disorders?
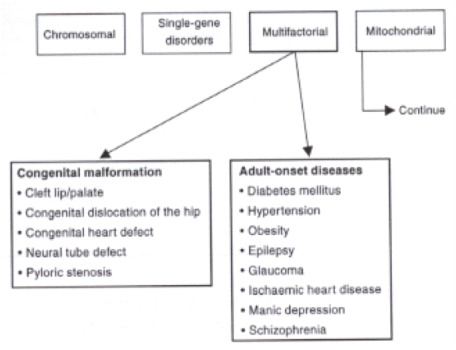
Multifactorial (or complex) disorders are conditions caused by a combination of both genetic and environmental/other factors. While researchers have learned that “nearly all conditions and diseases have a genetic component,” some are caused by mutations in a single gene, while others are caused by outside factors and are much more complex. Multiple gene mutations combined with lifestyle and environmental factors, such as drug/alcohol use or diet, result in multifactorial disorders such as Cleft Lip/Palate (1). While these disorders do occur more often in families, there is no explicitly defined pattern of inheritance, making risk factors and incidence hard to define. Since the causes of these disorders are extremely difficult to determine, multifactorial disorders are difficult to study and properly treat (5). These disorders can further be divided into congenital malformations, meaning malformations at birth, and adult-onset diseases.
What are Cleft Lip and Cleft Palate?
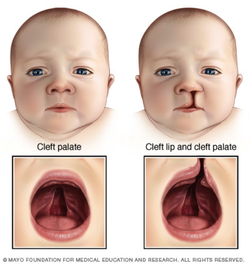
Cleft lip and cleft palate (CL/P) are some of the most common birth defects worldwide. Simply put, CL/P is a split in the mouth structure. A cleft lip can range from a small notch in the upper lip to a “split that can extend to the nose,” while a cleft palate (palate meaning “roof” of the mouth) can range from a “small malformation” to a large separation (3). There are three primary types of clefts: CL/P, isolated cleft palate, and isolated cleft lip. CL/P indicates that both the lip and palate are cleft – this condition makes up about 50% of all clefts and occurs most often in male children. The latter two clefts, isolated lip or palate, indicate just that: the cleft occurs only on the lip or palate. These occur about half as often as cleft lip and palate and occur more often in female children (3). Additionally, clefts are further classified as unilateral, a split on one side, or bilateral, one split on each side.
Causes, incidence, and risk factors
There are many causes to cleft lip and palate, these include genes passed down from one or both parents, or even environmental factors such as use of drugs or alcohol. Risk factors include family history of CL/P or other birth defects. However, since there are so many causes, it is difficult to name specific risk factors that may directly cause this congenital disorder. Globally, about 1 out of every 2,500 people will be born with a cleft palate. Having a cleft lip or palate can have a number of affects on an individuals’ life, including an effect on the appearance of a face, potential feeding and speech problems, and potentially reoccurring ear infections (2).
All humans actually start out with a cleft lip and palate when developing in the womb. Between the 6th and 11th week of pregnancy, the clefts in the lip and palate fuse together to form our faces. When a baby is born with a cleft lip or palate it simply indicates that the clefts failed to fuse while the child was developing in the womb (3).
Genetics Behind Cleft Lip/Palate
The genetics behind this disorder are complex, especially considering the causes are not explicitly known. Development of the head and face are some of the most complex events while the child develops in the womb. A network of transcription factors, signaling molecules, and proteins, conferring cell polarity and cell–cell interactions, coordinates them. Any disruption of this process can result in craniofacial abnormalities, including cleft lip and palate (2). Studies show that the majority of CL/P are regarded as non-syndromic, meaning they occur without other anomalies (2). The syndromic cases, those that occur with other anomalies, simply have additional characteristic features. These additional features are subcategorized into chromosomal abnormalities, both known and unknown (2). The study conducted by Philip Stanier and Gudrun Moore indicates that though non-genetic risk factors have been identified, advances are still being made to identify genetic causes of CL/P. Though there is progress in identifying environmental and genetic triggers for CL/P the etiology behind the genetic defects are still generally unknown, though extensive testing has been done on the genes of mice in hopes of locating specific genes that may be responsible for craniofacial abnormalities.
Symptoms
There are a number of symptoms physically and behaviorally for individuals with CL/P, and some children may have one or more additional birth defects along with CL/P. Physically, there may be a small notch in the lip; some may have complete splits from the lip to the nose causing change in nose shape, and poor teeth alignment. These symptoms may also result in feeding problems such as flow of milk through nasal passages, speech problems, poor growth and failure to gain weight. (3)
Treatment
When a child is still an infant, surgery to close the cleft lip is done – called CL/P Repair surgery may also be required later in life if the problem has had a major effect on the nose area. Continued follow-up may be needed throughout the child’s life. Most babies should heal without any major issues, though future surgeries may be needed to fix any remaining scars. Fortunately, as the surgery is done while the children are under one year old, issues with teeth may be dealt with later on during childhood as the teeth come in. Hearing and speech problems may still exist and speech therapy options should be considered for further treatment (3)
Causes, incidence, and risk factors
There are many causes to cleft lip and palate, these include genes passed down from one or both parents, or even environmental factors such as use of drugs or alcohol. Risk factors include family history of CL/P or other birth defects. However, since there are so many causes, it is difficult to name specific risk factors that may directly cause this congenital disorder. Globally, about 1 out of every 2,500 people will be born with a cleft palate. Having a cleft lip or palate can have a number of affects on an individuals’ life, including an effect on the appearance of a face, potential feeding and speech problems, and potentially reoccurring ear infections (2).
All humans actually start out with a cleft lip and palate when developing in the womb. Between the 6th and 11th week of pregnancy, the clefts in the lip and palate fuse together to form our faces. When a baby is born with a cleft lip or palate it simply indicates that the clefts failed to fuse while the child was developing in the womb (3).
Genetics Behind Cleft Lip/Palate
The genetics behind this disorder are complex, especially considering the causes are not explicitly known. Development of the head and face are some of the most complex events while the child develops in the womb. A network of transcription factors, signaling molecules, and proteins, conferring cell polarity and cell–cell interactions, coordinates them. Any disruption of this process can result in craniofacial abnormalities, including cleft lip and palate (2). Studies show that the majority of CL/P are regarded as non-syndromic, meaning they occur without other anomalies (2). The syndromic cases, those that occur with other anomalies, simply have additional characteristic features. These additional features are subcategorized into chromosomal abnormalities, both known and unknown (2). The study conducted by Philip Stanier and Gudrun Moore indicates that though non-genetic risk factors have been identified, advances are still being made to identify genetic causes of CL/P. Though there is progress in identifying environmental and genetic triggers for CL/P the etiology behind the genetic defects are still generally unknown, though extensive testing has been done on the genes of mice in hopes of locating specific genes that may be responsible for craniofacial abnormalities.
Symptoms
There are a number of symptoms physically and behaviorally for individuals with CL/P, and some children may have one or more additional birth defects along with CL/P. Physically, there may be a small notch in the lip; some may have complete splits from the lip to the nose causing change in nose shape, and poor teeth alignment. These symptoms may also result in feeding problems such as flow of milk through nasal passages, speech problems, poor growth and failure to gain weight. (3)
Treatment
When a child is still an infant, surgery to close the cleft lip is done – called CL/P Repair surgery may also be required later in life if the problem has had a major effect on the nose area. Continued follow-up may be needed throughout the child’s life. Most babies should heal without any major issues, though future surgeries may be needed to fix any remaining scars. Fortunately, as the surgery is done while the children are under one year old, issues with teeth may be dealt with later on during childhood as the teeth come in. Hearing and speech problems may still exist and speech therapy options should be considered for further treatment (3)
Critical Thinking Questions
1. What ethical issues (if any) might come up if parents learn their child has a cleft lip/palate while inside the womb?
2. What coping mechanisms would you prescribe to children with cleft lip/palate and their families?
2. What coping mechanisms would you prescribe to children with cleft lip/palate and their families?
Works Cited
1. Barlow-Stewart Kristine. “Environmental and Genetic Interactions – Complex Patterns of Inheritance 1.” The Australian Genetics Resource Book. June 2007. < http://www.genetics.edu.au/Information/Genetics-Fact-Sheets/Environmetal-and-Genetic-Interactions-Complex-Patterns-of-Inheritance1-FS11>
2. “Cleft Lip and Palate.” A.D.A.M. Medical Encyclopedia. PubMed Health. May 1, 2011 <http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002046/>
3. “Fact Sheet: Cleft Lip and Cleft Palate.” American Academy of Otolaryngology – Head and Neck Surgery. October 13, 2011. <http://www.entnet.org/HealthInformation/cleftLipPalate.cfm>
4. Stanier, Philip and Gudrun E. Moore. Human Molecular Genetics. Oxford Journals. Volume 13 Issue suppl 1. January 13, 2004 <http://hmg.oxfordjournals.org/content/13/suppl_1/R73.full>
5. What are complex or multifactorial disorders? Genetics Home Reference. November 25, 2012. <http://ghr.nlm.nih.gov/handbook/mutationsanddisorders/complexdisorders>
6. (Figure 1) El- Hazmi. M.A.F. Spectrum of Genetic Disorders and the Impact on Health Care Delivery: An Introduction. Islam Science Engineering and Technology. Bioethics. Genetic Engineering. <http://www.islamset.com/bioethics/genetics/images/figure2d.GIF>
7. (Figure 2) “Cleft Lip and Cleft Palate.” Mayo Clinic. Mayo Foundation for Medical Education and Research. <http://www.idahosurgicalarts.com/images/cleft_palate.jpg>
2. “Cleft Lip and Palate.” A.D.A.M. Medical Encyclopedia. PubMed Health. May 1, 2011 <http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002046/>
3. “Fact Sheet: Cleft Lip and Cleft Palate.” American Academy of Otolaryngology – Head and Neck Surgery. October 13, 2011. <http://www.entnet.org/HealthInformation/cleftLipPalate.cfm>
4. Stanier, Philip and Gudrun E. Moore. Human Molecular Genetics. Oxford Journals. Volume 13 Issue suppl 1. January 13, 2004 <http://hmg.oxfordjournals.org/content/13/suppl_1/R73.full>
5. What are complex or multifactorial disorders? Genetics Home Reference. November 25, 2012. <http://ghr.nlm.nih.gov/handbook/mutationsanddisorders/complexdisorders>
6. (Figure 1) El- Hazmi. M.A.F. Spectrum of Genetic Disorders and the Impact on Health Care Delivery: An Introduction. Islam Science Engineering and Technology. Bioethics. Genetic Engineering. <http://www.islamset.com/bioethics/genetics/images/figure2d.GIF>
7. (Figure 2) “Cleft Lip and Cleft Palate.” Mayo Clinic. Mayo Foundation for Medical Education and Research. <http://www.idahosurgicalarts.com/images/cleft_palate.jpg>
