Future Innovations of Cleft Lip and Palate
(Image 1)
A successful cleft lip or palate surgery faces many obstacles, including selecting the appropriate treatment for the patient, determining the appropriate age to begin treatment, the varying surgical techniques the surgeon can use, and changes to the surgical results as the patient grows and matures (1). Additionally, because each case is unique, the course of treatment is not always standard. However, over the years, advancements in the multidisciplinary reconstruction options have improved patients’ results, both physically and aesthetically (2). Furthermore, techniques have been improved to allow for fewer surgeries, shorter recovery time, and fewer risks to the patient (3). The success of the many treatment options can be measured in multiple ways—facial appearance, clarity of speech, hearing sharpness, and facial growth and development (4). Repair of a cleft lip or palate often requires the collective work of many—a plastic surgeon, an orthodontist, a speech pathologist, an oral surgeon, a neurosurgeon, and a genetic specialist (5).
Treatment

(Image 2)
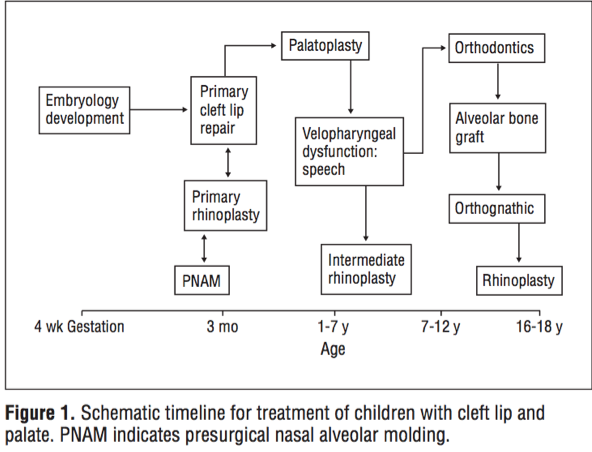
The treatment for the individual depends on the severity of the deformity, the presence of other birth defects, and the age of the patient (6). The reconstruction procedures occur at various points of age and development of the patient. Figure 1 illustrates the treatment options according to the age of the individual.
Presurgical
Advanced ultrasound technology now allows parents to begin preparing before their child is born. Prenatal consultations helps inform expectant parents about the difficulties they will face and what course of treatments to expect.
Since the 1950s, presurgical techniques such as lip taping, infant orthodontics, and maxillary arch devices have been developed and improved (6). Lip taping begins soon after birth. The taping helps alleviate the tension of the soft-tissue across the cleft. Presurgical nasal alveolar molding (PNAM), a form of preoperative orthopedics, is used in severe cases. PNAM usually begins when the child is six weeks old. PNAM helps reduce the width of the cleft and the soft tissue (7).
Surgical
Surgery is typically performed between two and three months of age, ideally at 10 weeks old. If the patient has a bilateral cleft lip or palate the surgery is more invasive and extensive and it may require two surgeries to repair and close the cleft (8).
Palatoplasty surgically reconstructs the palate using a prosthetic device, typically made out of an acrylic plate and wire. Palatoplasty closes the opening between the nose and mouth and improves speech, swallowing, eating, and breathing. The ideal age for a patient is between six and twelve months old. The repair of the soft and hard palate is performed between nine months and one year of age. After palatoplasty surgery, secondary speech surgery may be performed to improve velopharyngeal function. The velopharyngeal mechanism helps direct sound and air pressure in both the oral and nasal cavity.
Alveolar bone grafting is performed after the cleft palate is repaired in order to replace any missing bone from the front and roof of the mouth. The surgery is typically performed between eight and eleven years of age.
Orthodontic surgery, Rhinoplasty, and any other remaining cosmetic surgeries are the final step in the surgical process. An untreated nasal deformity that is a result of a cleft lip will worsen over time if it is not repaired (9).
New Innovations: Fetal Surgery
Over the past several decades, fetal surgery to repair congenital defects, such as cleft lip and palate, has been developed. Results show that successful fetal surgery outcomes result in less inflammation, scarring, and maxillary growth impairment. However, there is a 25% mortality rate of the fetus and the risks to the mother are very high as well. Currently, the International Fetal Medicine and Surgery Society only permits fetal surgery in situations that are life threatening and the prediction of surgical success after birth is poor (10).
Advanced ultrasound technology now allows parents to begin preparing before their child is born. Prenatal consultations helps inform expectant parents about the difficulties they will face and what course of treatments to expect.
Since the 1950s, presurgical techniques such as lip taping, infant orthodontics, and maxillary arch devices have been developed and improved (6). Lip taping begins soon after birth. The taping helps alleviate the tension of the soft-tissue across the cleft. Presurgical nasal alveolar molding (PNAM), a form of preoperative orthopedics, is used in severe cases. PNAM usually begins when the child is six weeks old. PNAM helps reduce the width of the cleft and the soft tissue (7).
Surgical
Surgery is typically performed between two and three months of age, ideally at 10 weeks old. If the patient has a bilateral cleft lip or palate the surgery is more invasive and extensive and it may require two surgeries to repair and close the cleft (8).
Palatoplasty surgically reconstructs the palate using a prosthetic device, typically made out of an acrylic plate and wire. Palatoplasty closes the opening between the nose and mouth and improves speech, swallowing, eating, and breathing. The ideal age for a patient is between six and twelve months old. The repair of the soft and hard palate is performed between nine months and one year of age. After palatoplasty surgery, secondary speech surgery may be performed to improve velopharyngeal function. The velopharyngeal mechanism helps direct sound and air pressure in both the oral and nasal cavity.
Alveolar bone grafting is performed after the cleft palate is repaired in order to replace any missing bone from the front and roof of the mouth. The surgery is typically performed between eight and eleven years of age.
Orthodontic surgery, Rhinoplasty, and any other remaining cosmetic surgeries are the final step in the surgical process. An untreated nasal deformity that is a result of a cleft lip will worsen over time if it is not repaired (9).
New Innovations: Fetal Surgery
Over the past several decades, fetal surgery to repair congenital defects, such as cleft lip and palate, has been developed. Results show that successful fetal surgery outcomes result in less inflammation, scarring, and maxillary growth impairment. However, there is a 25% mortality rate of the fetus and the risks to the mother are very high as well. Currently, the International Fetal Medicine and Surgery Society only permits fetal surgery in situations that are life threatening and the prediction of surgical success after birth is poor (10).
3D Computer Simulation
(Image 3)
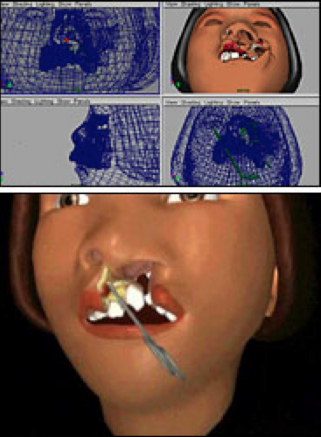
Animated simulations of cleft lip and palate surgeries have been developed that allow surgeons and medical students to practice surgical procedures and reconstructive techniques in a three dimensional environment that is highly accurate. This tool is beneficial for medical students to learn the approach of world-class surgeons and for surgeons to practice their skills. The images for the simulation were taken from real patients, using MRI and CT scans. The animation allows the viewer to see the surgical area from different views and angles, and allows them to virtually make incisions, remove layers of skin and tissue, and repair the area (11).
Operation Smile
(Image 4)
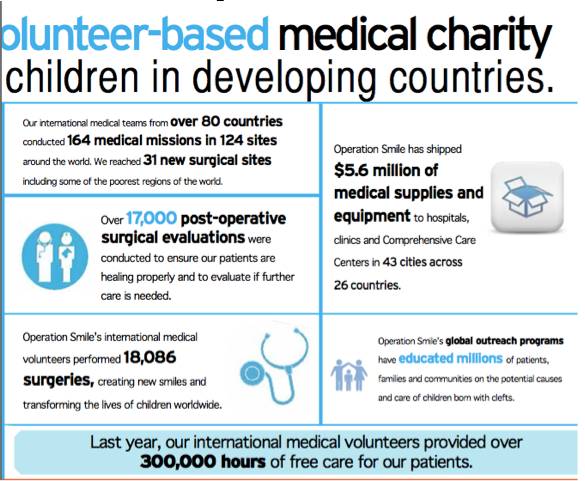
Operation Smile, which began in 1982, is dedicated to helping children internationally, who were born with a cleft lip or palate. Working in over 60 developing countries, Operation Smile provides reconstructive surgery for free to children will cleft lips, palates, and other facial deformities. Operation Smile has a huge presence worldwide, and with over 5,000 medical professionals from over 80 countries. They are able to provide treatment to individuals who would not otherwise have access to medical treatment or who could not afford it. Operation Smile has been expanding their outreach in countries and has been developing more and more medical sites across the world (12).
The Future
Previously, we had not been able to determine precisely which molecular events lead to the development of cleft lips and palates. However, genome sequencing has helped us to better identify specific genes related to the development of cleft lips and palates. Now that we have been able to determine specific genes that contribute to cleft lip and palate development, we will hopefully be able to gain an even better understanding of the genetic causations of cleft lips and palates (13). Genetic engineering and testing of cleft lips and palates will probebly face the same ethical and moral conflicts in the future that stem cell and cloning research have faced (14). Advances surgically, non-surgically, and technologically to repair cleft lip and palates continues today.
Critical Thinking Questions
1. Is fetal surgery morally and ethically right? Should parents be allowed to value the aesthetic results of their child over the potential fatal outcome? Should fetal surgical techniques be continued in order to improve their success rates and safety?
2. Is genetic engineering and testing of congenital malformations, such as cleft lip and palate, ethical?
The Future
Previously, we had not been able to determine precisely which molecular events lead to the development of cleft lips and palates. However, genome sequencing has helped us to better identify specific genes related to the development of cleft lips and palates. Now that we have been able to determine specific genes that contribute to cleft lip and palate development, we will hopefully be able to gain an even better understanding of the genetic causations of cleft lips and palates (13). Genetic engineering and testing of cleft lips and palates will probebly face the same ethical and moral conflicts in the future that stem cell and cloning research have faced (14). Advances surgically, non-surgically, and technologically to repair cleft lip and palates continues today.
Critical Thinking Questions
1. Is fetal surgery morally and ethically right? Should parents be allowed to value the aesthetic results of their child over the potential fatal outcome? Should fetal surgical techniques be continued in order to improve their success rates and safety?
2. Is genetic engineering and testing of congenital malformations, such as cleft lip and palate, ethical?
References
(1) Guerrero, Cesar A. "Cleft Lip and Palate Surgery: 30 Years Follow-up." Annals of Maxillofacial Surgery 2.2 (2012): 153-57. Print.
(2) Tollefson, T. T., C. W. Senders, and J. M. Sykes. “Changing Perspectives in Cleft Lip and Palate: From Acrylic to Allele.” Archives of Facial Plastic Surgery 10.6 (2008): 395-400. Print.
(3) Holsinger, F., D. Goldenberg, R. Levin, H. Macapinlac, D. Trask, and G. Harel. “Integrated PET/CT in Head and Neck Cancer: Controversies and Challenges.” Otolaryngology - Head and Neck Surgery 139.2 (2008): P18. Print.
(4) “Research and Innovations.” Nationwide Children's Hospital. N.p., n.d. Web. 15 Nov. 2012. <http://www.nationwidechildrens.org/cleft-lip-palate-research>.
(5) Habal, Mutaz B., MD. "Getting Clefts to the Forefront of Plastic Surgery, Based on New Innovation and Advances: The Crusaders of the Lost Ark." Editorial. THe Journal of Craniofacial Surgery Jan. 2009: 1-2. Print.
(6) "Facts about Cleft Lip and Cleft Palate." Centers for Disease Control and Prevention. N.p., 19 July 2012. Web. 01 Dec. 2012. <http://www.cdc.gov/ncbddd/birthdefects/cleftlip.html>.
(7) Tollefson, et al.
(8) Lydiatt DD, Yonkers AJ, Schall DG (November 1989). "The management of the cleft lip and palate patient". Nebr Med J 74 (11): 325–8; discussion 328–9.
(9) Tollfsson, et al.
(10) Shaffer, Amanda. "Cleft Palate Practice, Pre-Surgery." The New York Times. N.p., 2 Aug. 2005. Web. 1 Dec. 2012. <http://www.nytimes.com/2005/08/02/health/02clef.html?pagewanted=all>.
(11) "2011 Annual Impact Report." Operation Smile. N.p., 2011. Web. 1 Dec. 2012. <http://www.operationsmile.org/downloadables/news-events/publications/2011-annual-report.pdf>.
(12) Stanier, Philip, and Gudrun E. Moore. "Genetics of Cleft Lip and Palate: Syndromic Genes Contribute to the Incidence of Non-syndromic Clefts." Human Molecular Genetics 13.1 (2004): R73-81. Print.
(13) Tollefson, et al.
(14) Guerrero, et al.
(15) Tollefson, et al.
Image 1- "2011 Annual Impact Report." Operation Smile. N.p., 2011. Web. 1 Dec. 2012. <http://www.operationsmile.org/downloadables/news-events/publications/2011-annual-report.pdf>.
Image 2-https://secure.operationsmile.org/site/Donation2?df_id=12700&12700.donation=form1&utm_source=google&utm_medium=cpc&utm_term=operation%20smile&utm_campaign=paid
Figure 1- Tollefson, T. T., C. W. Senders, and J. M. Sykes. “Changing Perspectives in Cleft Lip and Palate: From Acrylic to Allele.” Archives of Facial Plastic Surgery 10.6 (2008): 395-400. Print.
Image 3- Shaffer, Amanda. "Cleft Palate Practice, Pre-Surgery." The New York Times. N.p., 2 Aug. 2005. Web. 1 Dec. 2012. <http://www.nytimes.com/2005/08/02/health/02clef.html?pagewanted=all>.
Image 4- "2011 Annual Impact Report." Operation Smile. N.p., 2011. Web. 1 Dec. 2012. <http://www.operationsmile.org/downloadables/news-events/publications/2011-annual-report.pdf>.
(1) Guerrero, Cesar A. "Cleft Lip and Palate Surgery: 30 Years Follow-up." Annals of Maxillofacial Surgery 2.2 (2012): 153-57. Print.
(2) Tollefson, T. T., C. W. Senders, and J. M. Sykes. “Changing Perspectives in Cleft Lip and Palate: From Acrylic to Allele.” Archives of Facial Plastic Surgery 10.6 (2008): 395-400. Print.
(3) Holsinger, F., D. Goldenberg, R. Levin, H. Macapinlac, D. Trask, and G. Harel. “Integrated PET/CT in Head and Neck Cancer: Controversies and Challenges.” Otolaryngology - Head and Neck Surgery 139.2 (2008): P18. Print.
(4) “Research and Innovations.” Nationwide Children's Hospital. N.p., n.d. Web. 15 Nov. 2012. <http://www.nationwidechildrens.org/cleft-lip-palate-research>.
(5) Habal, Mutaz B., MD. "Getting Clefts to the Forefront of Plastic Surgery, Based on New Innovation and Advances: The Crusaders of the Lost Ark." Editorial. THe Journal of Craniofacial Surgery Jan. 2009: 1-2. Print.
(6) "Facts about Cleft Lip and Cleft Palate." Centers for Disease Control and Prevention. N.p., 19 July 2012. Web. 01 Dec. 2012. <http://www.cdc.gov/ncbddd/birthdefects/cleftlip.html>.
(7) Tollefson, et al.
(8) Lydiatt DD, Yonkers AJ, Schall DG (November 1989). "The management of the cleft lip and palate patient". Nebr Med J 74 (11): 325–8; discussion 328–9.
(9) Tollfsson, et al.
(10) Shaffer, Amanda. "Cleft Palate Practice, Pre-Surgery." The New York Times. N.p., 2 Aug. 2005. Web. 1 Dec. 2012. <http://www.nytimes.com/2005/08/02/health/02clef.html?pagewanted=all>.
(11) "2011 Annual Impact Report." Operation Smile. N.p., 2011. Web. 1 Dec. 2012. <http://www.operationsmile.org/downloadables/news-events/publications/2011-annual-report.pdf>.
(12) Stanier, Philip, and Gudrun E. Moore. "Genetics of Cleft Lip and Palate: Syndromic Genes Contribute to the Incidence of Non-syndromic Clefts." Human Molecular Genetics 13.1 (2004): R73-81. Print.
(13) Tollefson, et al.
(14) Guerrero, et al.
(15) Tollefson, et al.
Image 1- "2011 Annual Impact Report." Operation Smile. N.p., 2011. Web. 1 Dec. 2012. <http://www.operationsmile.org/downloadables/news-events/publications/2011-annual-report.pdf>.
Image 2-https://secure.operationsmile.org/site/Donation2?df_id=12700&12700.donation=form1&utm_source=google&utm_medium=cpc&utm_term=operation%20smile&utm_campaign=paid
Figure 1- Tollefson, T. T., C. W. Senders, and J. M. Sykes. “Changing Perspectives in Cleft Lip and Palate: From Acrylic to Allele.” Archives of Facial Plastic Surgery 10.6 (2008): 395-400. Print.
Image 3- Shaffer, Amanda. "Cleft Palate Practice, Pre-Surgery." The New York Times. N.p., 2 Aug. 2005. Web. 1 Dec. 2012. <http://www.nytimes.com/2005/08/02/health/02clef.html?pagewanted=all>.
Image 4- "2011 Annual Impact Report." Operation Smile. N.p., 2011. Web. 1 Dec. 2012. <http://www.operationsmile.org/downloadables/news-events/publications/2011-annual-report.pdf>.
